

Introduction
According to the Institute of Medicine of the National Academies, pain affects more Americans than diabetes, heart disease and cancer combined [1]. Pain is a significant public health problem that costs society at least $560-$635 billion annually. Adoption of pain medications and safe healthcare practices is a major global policy concern. As such we need to ensure that the right patients are getting the correct medicine prescribed by the right doctor. Pain medications are prescribed by multitude of physicians from different specialties. However, adoption of pain medication is a lively process that is highly dependent on the interpersonal interactions between members of a social network.
Social Network Analysis (SNA)[2], which views the structure of social interactions as networks composed of nodes (physicians) interconnected by edges (social relations, friendship, advice), is an ideal approach for describing interaction patterns to study how social influence is transmitted among physicians and how it affects their contingent behavior [3]. A social network/system is the pattern of friendship, advice, communication or support which exists among the members of a social system. Social network analysis can help us better understand complex interactions at different levels between its members. Such networks can be used to find key-opinion leadersinside a social system. Key opinion leadersare people or organizations that have a strong social influence and are perceived to be knowledgeable and proficient in their area.
Whenever a new pain medication is released, the adoption process in a social network is unlikely to be simultaneous, i.e., not all physicians adopt the medication at the same time [3]. For many new medications, an individual’s decision to adopt the medicine depends on whether his contacts have adopted it already. The adoption processmay differ from one individual to another. While some may adopt the innovation early, others may adopt it late or may not adopt it at all. The adoption processes are also affected by key opinion leaders. Their recommendations and opinions are highly sought after and listened to when making important decisions.
Existing applications of SNA for investigating the adoption of an innovation among physicians have been hospital-specific, and they relied on physicians’ self-reports [4-5]. However, these models suffer from sampling bias that is inherent in their hospital-centric data collection. The physician may underestimate or overestimate their social contacts and also may be hesitant to disclose personal information. Also, data regarding physician’s social network is not freely available. A physician’s social network will help us understand the underlying dynamics of the network, which can help us disseminate information more efficiently. Thus, SNA research that considers many physicians over several hospitals in a geographic area and that is independent of physician’s self-reports is much needed. In this paper, using big-data and data-mining, we create a social network of several physicians over a number of hospitals in the US by considering assumptions on physician’s specialty and affiliation to the same hospital. We then using graph centrality measures and prescription volume to find key-opinion leaders in the social network.
Methodology
In our work [6], we create a social network by mining big-data from 30+ hospitals and 2000+ physicians from the eastern part of USA. We used a medical-prescriptions dataset and the Healthcare Organization Services (HCOS) [7] physician-affiliation dataset to create a social network of physicians prescribing pain medications. The prescription dataset consisted of billions of physicians in the US prescribing certain pain medications between years 2005 and 2017. Then, using the prescription data of these physicians, we create a directed influence graph for identifying the key opinion leaders using degree (in-degree and out-degree). Since the influence graph is directed, in-degree of a node signifies the number of edges that are directed towards the node and out-degree signifies the number of edges that are going out from the node. Degree centralitymeasures the in-degree and out-degree of a node. This was used as a measure of importance and influence in our social network.
To form the social network, the following assumptions are used: Physicians affiliated or working in the same hospital within the same specialty or specialty group and prescribing the same pain medication are assumed to influence each other. Although we assumed as per above, there are several other assumptions possible that one could explore. Specialty groups are like clusters that contain specialties from similar fields that are related to one another. Once the social network is created using the above assumptions, we use the adoption pattern for a popular pain-medication (called M) to create a directed influence graph. A directed influence graph is a directed graph where the direction of edge defines the direction from where the influence propagated. The time of first prescription of the pain medication by a physician is taken as the time of adoption of the innovation by the physician. Physicians adopting M on a certain date are assumed to influence other physicians’ adoption of M in his/her social network after this date. In the directed graph, an arrow (A, B) is directed from A to B, where ‘A’ signifies the physician that has been influenced by physician ‘B’ for medication’s adoption.
Results
We found that physicians from specialty internal medicine and family medicine had the highest in-degree (see Fig. 1). High in-degree centrality for a physician signify that the physician has influenced more number of physicians in his/her social network. Next, we analyzed the total number of scripts of medicine M prescribed by each physician. We found that even though physicians from specialties internal medicine and family medicine were highly influential (high in-degree, see Fig. 1); neurology and nurse practitioners were the ones prescribing the highest volumes of medication M (see Fig. 2).
Next, we analyzed the demographic data (gender) of the physicians. We found that number of males (16) and female (15) physicians prescribing the medication M were similar; however, females (mostly nurse-practitioners) were prescribing higher volume of scripts compared to male physicians (males: 132,004; females: 159,361).
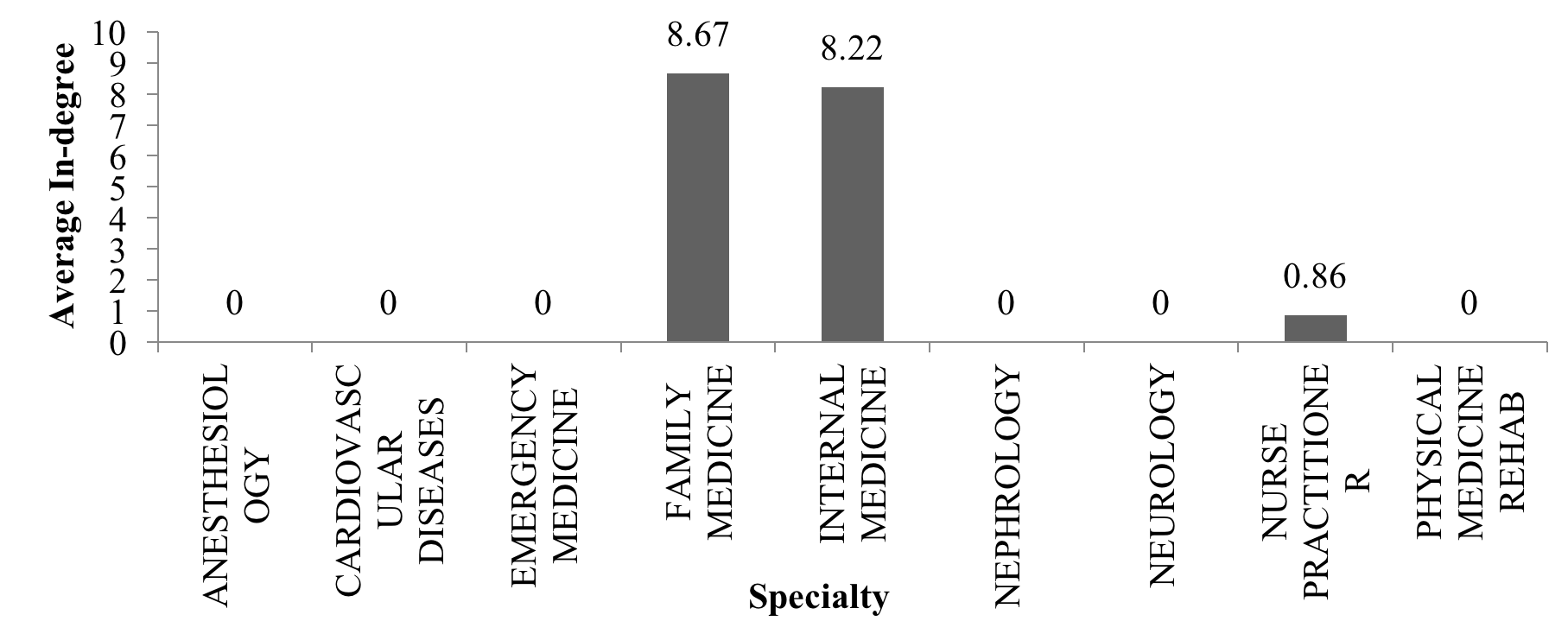
Fig. 1. Average In-degree for different specialties. Source: [6]
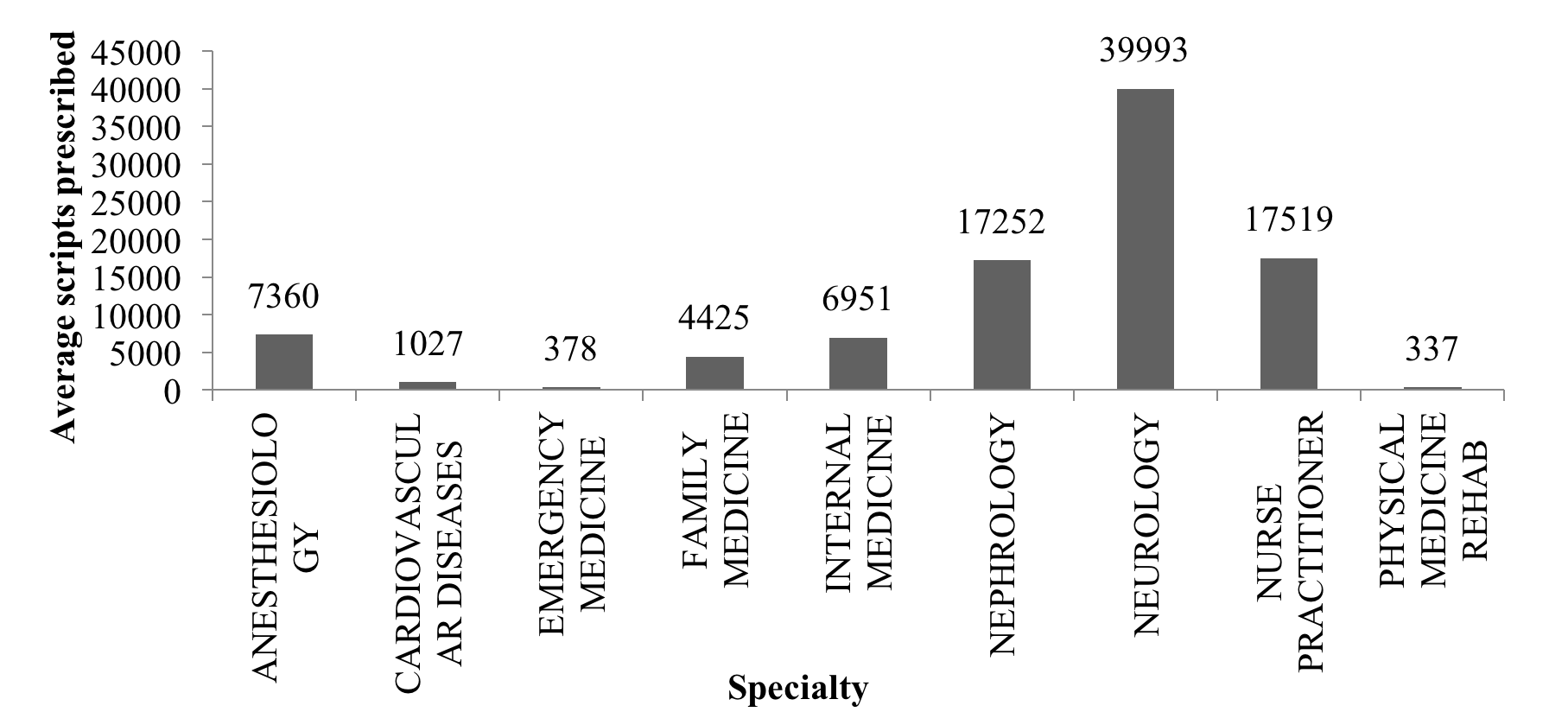
Fig. 2. Average number of scripts prescribed per specialty. Source: [6]
Conclusion
Our results reveal that physicians with specialties family medicine and internal medicine were highly influential in the diffusion of pain medication within their social network (see Fig 1). One likely reason for this result could be that physicians with these specialties are primary-care providers(PCPs), who are the first point-of-contact for any undiagnosed pain issues reported by patients. These PCPs know many other specialties as they are in the process of regularly referring patients to these specialties. We also found that nurse practitioners and neurologists were prescribing more scripts of pain medication than other specialties (see Fig 2). One likely reason for this observation could be that Nurse practitionersare trained to manage acute and chronic medical conditions [8]. Thus, they come in contact with a greater number of patients suffering from pain as compared to the physicians from other specialties. Finally, our results show that female physicians were prescribing more scripts of pain medication as compared to males. Upon investigation, we found that this can be attributed to the fact that Nurse practitioners were mostly females and since they were prescribing high number of scripts of the medicine, the prescription volume was skewed towards female physicians as compared to male physicians.
In hindsight, we conclude that Primary-Care Physicians (PCPs) with specialties like family medicine and internal medicine are the most influential doctors prescribing pain medications. However, these PCPs are not among the highest volume prescribers of the pain medications
This work has been published in the Proceedings of the 2017 IEEE/ACM International Conference on Advances in Social Networks Analysis and Mining 2017.
Acknowledgement
We are grateful to Nataraj Dasgupta, Baskaran Sankaran, Madeline Coleman, and Susanna Helton for their kind comments and feedback on a draft version of this article.
References
[2] Scott, J.: Network Analysis: A Handbook. Sage. Newbury Park, CA (1991)
